A seventeen year old defensive linebacker falls down during football practice. He isn’t breathing. Seven minutes later the EMTs are on scene. A sixteen year-old guard collapses while playing pickup basketball with his friends. He’s unresponsive and rushed to a nearby hospital. An eighteen year old basketball player collapses mid game. Paramedics treat him five minutes later. By the time he makes it to the hospital he is placed on life support. A sixteen year old swimmer stops mid-stroke, sinking to the tiled black strip of the pool floor. She’s not breathing when her teammates pull her from the water. Her coach runs for the pool deck defibrillator.
All four of these stories are real. All four of these patients displayed no prior symptoms. All four went into cardiac arrest. Only one survived.

Cardiac arrest is an abrupt loss of heart function that is often fatal if appropriate action for treatment is not immediately taken. Nine out of ten cardiac arrest events occur outside of a hospital setting with only a 5-10% change of survival (Fig 1). Cardiac arrest is the leading cause of death in athletes and sport-related cardiac arrest accounts for nearly 39% of all cases in adolescents. Male athletes are at a greater risk than female athletes. The difference in risk between men and women is often attributed to the protective effects of the sex hormone estrogen. African American athletes are at a much higher risk for cardiac arrest in sports. Cardiac arrest is more common in sports with high levels of exertion such as basketball, soccer, and hockey. The American College of Cardiology estimates between 100 to 150 sudden cardiac arrest cases during competitive sports result in sudden death each year.
Isn’t Cardiac Arrest Another Word for Heart Attack?
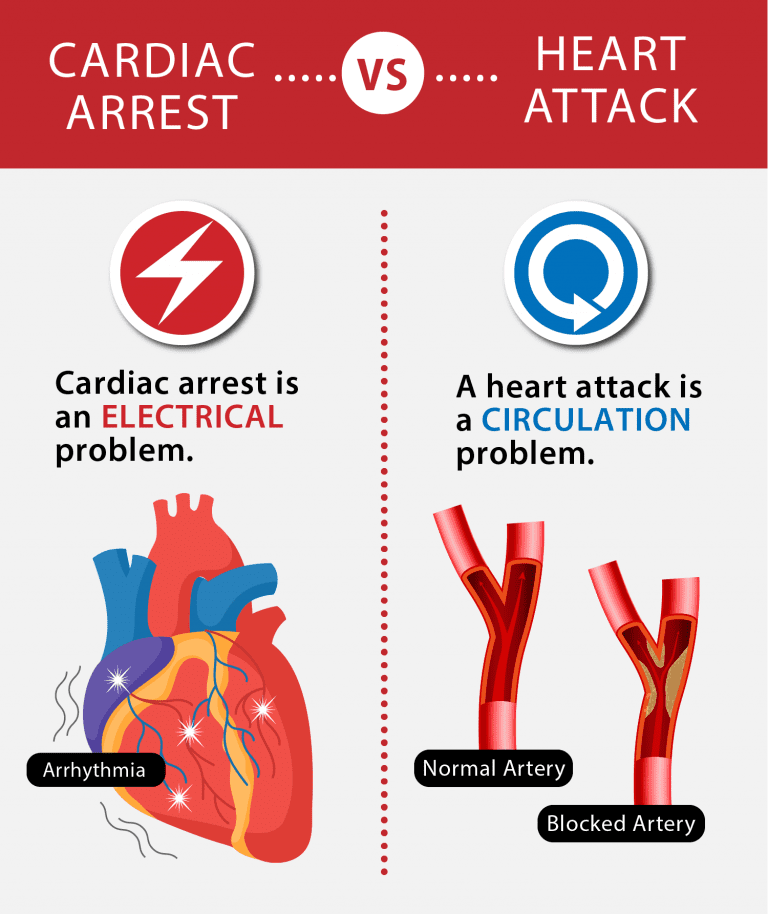
Cardiac arrest and a heart attack are commonly thought to be the same thing. This misconception is often why cardiac arrest signs are misinterpreted for a heart attack. However, a heart attack and cardiac arrest are quite different. A heart attack occurs when there is a blockage of blood flow to the heart. Cardiac arrest is a result of an electrical malfunction which “arrests” the heart’s ability to pump blood (Fig 2). Ventricular fibrillation is the most common electrical malfunction preceding cardiac arrest as the heart’s lower chambers quiver instead of contracting normally.
A heart attack may cause cardiac arrest, but not all cardiac arrest cases are a result of a heart attack. Signs of a heart attack may be immediate, or start slowly with mild symptoms. It’s also possible to have a heart attack without any symptoms. Nearly 1 in 5 heart attacks are silent. Heart attack symptoms can vary between men and women. However, unlike a heart attack, cardiac arrest symptoms are never silent and don’t present with differences between men and women (Fig 3).
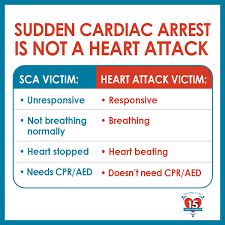
During cardiac arrest, the heart completely stops beating. Blood is stagnant and is no longer pumped throughout the body nor to the brain. Thus, the person suddenly passes out and will appear lifeless. In some cardiac arrest cases, victims may experience 10-20 seconds of seizure activity as the brain stops receiving blood and oxygen. People in cardiac arrest will never awaken independently and always need immediate medical attention.
Why Does Cardiac Arrest Present in “Healthy” Athletes?
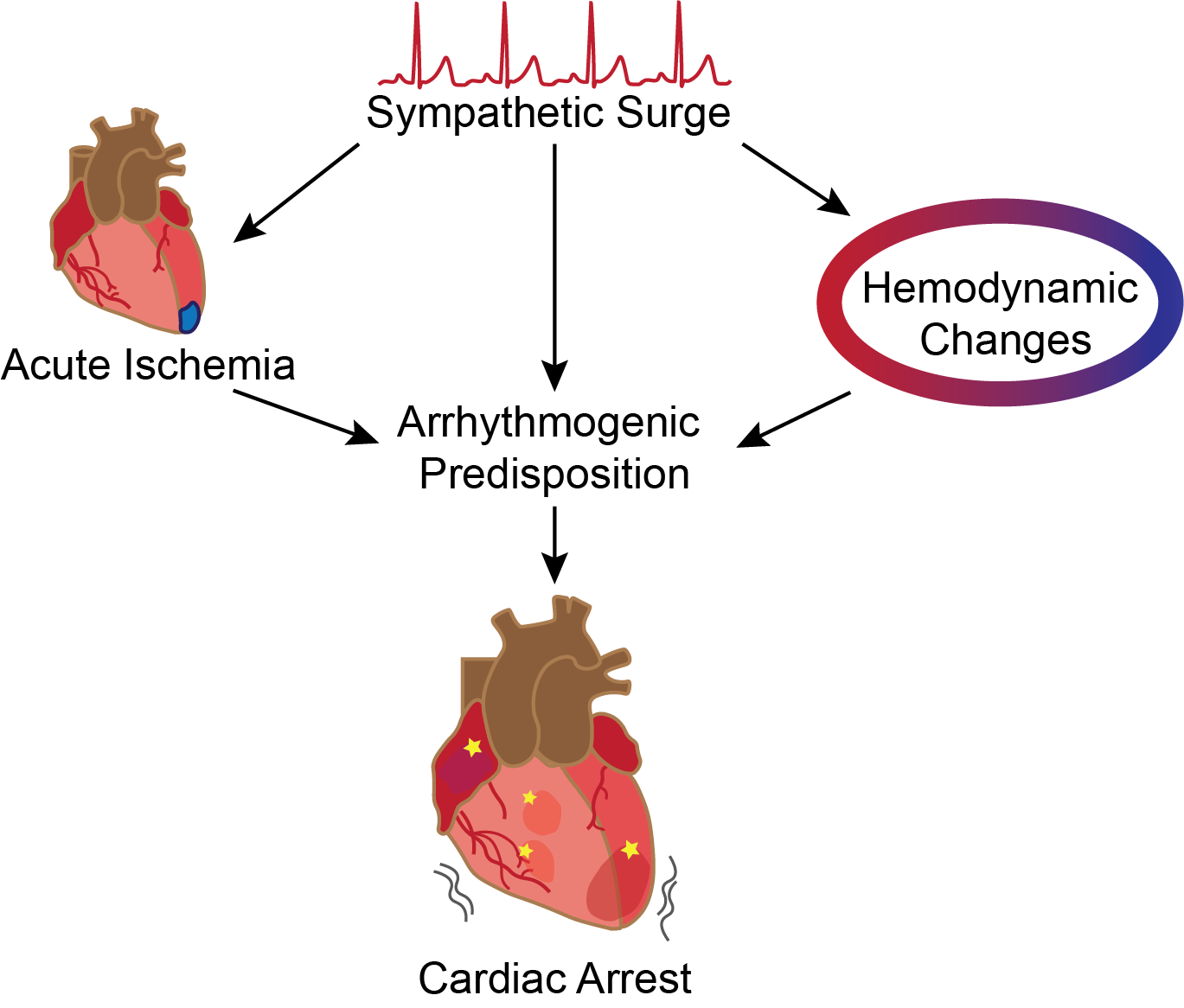
Cardiac arrest in athletes is traumatic as seemingly healthy athletes collapse in front of a crowd. Why is it that athletes, often at the middle to height of their athletic careers, suffer from cardiac arrest on the field? The answers vary. The heart must work harder in high activity sports such that the risk of suffering cardiac arrest is 10 times higher for predisposed athletes. Exercise produces an increased demand for oxygen, activates the sympathetic nervous system, and alters the heart’s hemodynamics, the patterns of blood flow (Fig 4). Abrupt changes to any of these three factors, coupled with an arrhythmogenic event can lead to cardiac arrest. Most often, cardiac arrest during a high activity sporting event occurs without any prior symptoms or warning signs, despite possible underlying conditions. The cause of cardiac arrest cases for athletes under 35 falls into two categories: structural abnormalities and electrical abnormalities.
Of the various cardiac structural abnormalities, hypertrophic cardiomyopathy (HCM) is the leading cause of cardiac arrest in athletes. HCM can be confused with “athlete’s heart” as both display cardiac hypertrophy or muscle enlargement. The increase in heart mass in athlete’s heart is an adaptive change to intense cardiovascular training. HCM, however, is a result of genetic mutations that impact the cardiac muscle. Enlargement of the heart’s lower chamber, or ventricle, leads to an elevated risk for tachycardia and ventricular fibrillation during high activity sports. Blood vessel abnormalities may also lead to cardiac arrest as a result of adrenaline release during physical activity. Coronary artery anomalies, narrow arteries within and around the heart, are the second leading cause of cardiac arrest. While HCM is the most common cause of sports related cardiac arrest in the US, Arrhythmogenic Right Ventricular Cardiomyopathy (ARCV) is the most common cause of cardiac arrest in Europe. ARVC is a genetic disease characterized by arrhythmias and ventricular dysfunction where exercise increases the risk for cardiac arrest 5-fold. An ARVC diagnosis is one of the only diseases that results in mandatory exclusion from high intensity sports and forced retirement.
In structurally normal hearts, electrical abnormalities are the most likely cause of cardiac arrest. Electrical abnormalities aside from known arrhythmias include diseases such as Long QT Syndrome and Wolff-Parkinson-White syndrome. Inflammation of the heart muscle (myocarditis) and vessels (Kawaski’s disease) are known to result in electrical abnormalities and in some cases lead to cardiac arrest during sports.
Cardiac arrest during sports may also be the result of commotio cordis, which was the cause of Buffalo Bills safety Damar Hamlin’s cardiac arrest on January 2nd of this year. Only 10 to 20 commotio cordis cases occur annually, as there is a moment less than one fifth of a second during the cardiac rhythm cycle where the heart is susceptible to projectile force. A hard hit to the left side of the chest, often caused by a baseball, hockey puck, or lacrosse ball disrupts the electrical cycle and results in cardiac arrest.
Over 80% of athletes who suddenly die from cardiac arrest have no symptoms or family history. Preventing cardiac arrest in athletes is challenging as most people are unaware they have any predisposing conditions. Both the American Heart Association and European Society of Cardiology recommend screening for all athletes that participate in high level sports. Heart screening and diagnostic tests with an electrocardiogram (ECG) can detect some of these conditions. However, ECG results of an athlete’s heart are different from the results of an average person. This discrepancy has led to a small number of false-negative and false-positive results (<5%). While preparticipation screening for young competitive athletes remains controversial, cardiac screening remains the only method for detecting cardiac abnormalities in athletes that could cause cardiac arrest.
Life-saving Actions for Cardiac Arrest Victims: The 911, CPR, and AED Trifecta

If you see a person with symptoms of cardiac arrest, immediately call 911. Do not hesitate. The quicker the emergency medical services are notified of a cardiac arrest event, the sooner they can be on the scene. Be clear and to the point when talking to the operator. The American Heart Association recommends using simple, direct language: “Heart stopped, I need help.” Begin cardiopulmonary resuscitation, better known as CPR. CPR compressions act as an external heart. With each compression, blood is “pumped” throughout the body to the brain and vital organs. Every minute a person goes without blood to the brain risks serious neurological damage. Performing hands-only CPR doubles or triples chances of survival (Fig 5).
To perform CPR, place your palms on the center of the chest and press down hard and fast. The chest bone should drop at least two inches for teenagers and adults. For speed, the goal is 100 to 120 beats per minute (bpm). Both the New York Presbyterian Hospital and American Heart Association have made Spotify playlists of songs with beats over 100 bpm. Composed of a variety of genres and artists, from Gaga’s “Just Dance” to the All American Rejects’ “Gives you Hell” to “Stayin’ Alive” by Bee Gees, all the songs in the playlist have a tempo between 100 and 120 bpm. Pick one, memorize it, and hum it while giving chest compressions.
Finally, use an automated external defibrillator or AED if one is available. AEDs are often found in public spaces such as airports, offices, and schools. An AED is a portable, sophisticated medical device that analyzes the heart’s rhythm and delivers an electrical shock to the heart if appropriate. AEDs are also extremely easy to use with audible prompts and graphical directions. Anyone can use an AED. First turn the AED on and apply the defibrillator pads to the person’s bare chest. The AED will automatically analyze the patient’s cardiac rhythms to determine if there are “shockable rhythms.” If a shockable rhythm is detected the AED will deliver a “defibrillatory” electrical shock. If not, the AED will instruct the rescuer to continue performing CPR.
If there is more than one person on the scene, divide and conquer. One person should call 911 and perform CPR while the other looks for an AED. Activating the emergency response and starting CPR can be simultaneous. The worst thing to do during a cardiac arrest situation is to do nothing. Although CPR and AED administration can be the difference between life and death, many bystanders fail to act quickly when seeing a collapse. The readiness to perform CPR on women and minority groups is substantially lower. Further, bystanders worry chest compressions may break ribs or that they may hurt the person while administering CPR/AED. However, a person in cardiac arrest is clinically dead. Any actions made are life-saving and can only help. Good Samaritan laws provide civil immunity for good faith rescuers who use an AED in emergency situations across the US. Both bystander CPR and dispaster EMT-CPR is associated with higher survival outcomes and neurological function following and out of hospital cardiac arrest.
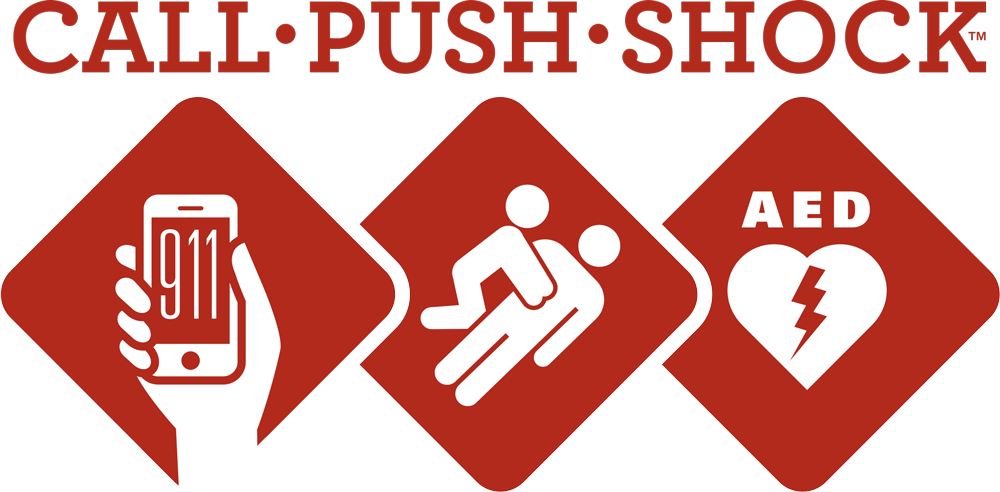
In summary, don’t hesitate: Call 911, begin CPR, and use an AED if one is available (Fig 6).
An Outlook for Cardiac Arrest Prevention
Damar Hamlin survived cardiac arrest thanks to the quick response of the Buffalo Bills Athletic Training staff and on-site medical team. The televised defibrillation given by the AED on January 2, 2023 made all the difference. Every minute that passes without defibrillation increases mortality by 10%. Hamlin’s survival is a miracle. Cartier Woods was not as lucky. On January 31, 2023, only 19 days after Hamlin, Woods went into cardiac arrest during a high school basketball game. There was no AED on site. Although paramedics arrived 10 minutes later to provide assistance, Woods was placed on life support and passed away on February 6, 2023.
Cardiac arrest prevention and survival depends on awareness, accessible cardiac screenings, and equitable access to AEDs. Currently only 24 of the 50 States require AEDs installed on school grounds. Of those, only California, Connecticut, Kentucky, Maine, and Massachusetts mandate AEDs be present at school athletic events. Two out of every fifty high schools can expect a cardiac arrest event on campus each year, yet nearly 35 million students from K through 12 attend schools in the US with no legal requirement for an onsite AED.
The demand for cardiac arrest awareness and accessible AEDs is often led by parents who have lost a child to cardiac arrest. The Play for Jake Foundation founded by the parents of Jacob West provides free cardiac screenings to adolescents and donates AEDs to schools across Indiana. The parents of Michael Ellssear advocated the Massachustets state legislator for Michael’s Law which passed in 2012 and mandates all public schools have a written emergency response plan and accessibility to an AED. The Eric Paredes Save a Life Foundation provides free cardiac screenings to high school students in California. The foundation has also placed over 190 AEDs in San Diego County and advocated for three sudden cardiac arrest laws that have been signed into California Law.
Studies have shown AED placement in schools increases survival following cardiac arrest to nearly 70%. Given this increase in survival, school based AED programs should be highly encouraged. AEDs are expensive, running between $1000 to $3000 depending on the model, and the cost can be a barrier for schools to purchase these life saving devices. Cost is not an excuse when it’s a matter of life and death. There can be nothing worse than explaining to the family of a cardiac arrest victim that their school was unprepared to save the life of their teenager. Increasing AED access and education is paramount to reducing the lives that cardiac arrest takes each year.
Cardiac arrest can happen to anyone, anywhere, at any time. Emergency training courses provide people with the skills to confidently read emergency situations and act accordingly until first responders arrive. The Red Cross and American Heart Association have online resources, classes, and certification courses for CPR/AED training. Red Cross offers flexible in person training for First Aid, CPR/AED and life support. Although not mandated by North Carolina law, UNC-Chapel Hill is equipped with over 100 AEDs across campus. They can be located on this map. To prepare for emergency readiness, Carolina provides free CPR classes and training every semester for students, staff, and faculty. Take action and be prepared. The difference in survival following cardiac arrest could very well be you.
Don’t let Cardiac Arrest steal your heart or your life! Make sure you know where the closest AED is to you and consider getting a defibrillator for your home! #cardiacarrest #cardiology #aed #defibrillator #humor #funny #meme #cartoon #DoYouSeeAnAED #WhereInTheWorldIsElliot pic.twitter.com/4yeUZPW9T4
— HeartHero 💔+⚡️= ❤️🩹 (@HeartHeroAED) April 29, 2020
Peer Editor: Whitney Bell