Consider a person who, years after a car accident, still grips the door handle when going around a curve and flinches at the sound of sirens. The crash they experienced is over; they know it is over. They can describe it, contextualize it, and even joke about it. Yet, at night the dreams still come. In traffic, their heart rate climbs and their jaw tightens. Understanding what happened and talking through the fear, anxiety, and anger has not changed how their body responds. This gap — between what the mind understands and what the body still does — sits at the center of a growing body of research into trauma, chronic diseases, and the limits of purely cognitive approaches to healing. Every person who lives through a traumatic event, and most people will, deserves to understand how trauma affects their biology and to have access to resources to support their healing.
For much of the twentieth century, the approach to healing psychological trauma was cognitive, which involved naming the experience, constructing a narrative about it, and then gaining insight that would then hopefully lead to the resolution of mental and physical distress. There are many forms of talk therapy, most of which assume that analysis of the emotions can reduce adverse symptoms. And while this is true for many difficulties, there is a growing body of research that is uncovering something more fundamental: trauma is not the external event itself, but rather the biological processes, or lack thereof, that lead to the development of psychological and physiological ailments. The effects of trauma can persist beyond conscious understanding in the form of dysregulation across multiple biological systems — including the stress response, autonomic nervous system, immune function , and the digestive system. The gap between what the mind understands and what the body continues to do may be one of the most consequential and least examined aspects of how we approach healing in conventional health care.

To begin to understand how that gap forms, it is important to look at what happens during a threatening experience. When the body detects danger, the nervous system responds almost instantly, increasing the heart rate, priming muscles for action, and narrowing attention before conscious thoughts form. This cascade of physiological events — commonly described as “fight, flight, or freeze”— unfolds faster than reasoning and largely bypasses language-based processing. A person does not decide to be frightened; rather, the body has already responded by the time conscious awareness catches up.
The nervous system is built to respond to threat, and once the danger has passed, it returns to baseline. In most cases, that response — or the surge of energy the body summoned to protect itself — naturally resolves, allowing the nervous system to reset. However, in some situations, that response does not fully resolve and some of the energy the body summoned lingers, leaving the nervous system unable to return to its pre-threat baseline. This can happen in situations where a person cannot escape, act, or recover in a way that allows the response to fully complete. For example, a child in an unsafe home may be unable to leave or fend for themselves, making a freeze or dissociated response the safest option available; a student being bullied may have to repeatedly flee from their aggressors, living with the fear of it happening again the next day; and a person in a car accident may have to suppress their own shock in order to take immediate action and help those around them. Under these unfortunate circumstances, that protective surge of energy has no clear path for resolution. The result can be a nervous system that continues operating as though danger is present, contributing to post-traumatic stress disorder (PTSD), which includes persistent hypervigilance, avoidance tendencies, and flashbacks, as well as broader health outcomes such as chronic pain, depression, and anxiety. These are not signs of weakness or poor coping. Peter Levine, biophysicist and psychologist, describes these symptoms as manifestations of an unfinished trauma response, in which the body has not fully processed or discharged the energy generated during the threat and remains in a state that is unable to register that the danger has passed. Levine developed his therapeutic model, Somatic Experiencing, around this idea.
There is substantial evidence supporting the idea that sustained physiological activation of the stress response carries long-term health consequences. Large studies, including the Adverse Childhood Experiences (ACE) Study, have found that early adversity is associated with increased risk of both psychiatric and physical illness in adulthood, including heart disease, neuropsychiatric symptoms, autoimmune conditions, and chronic pain. This suggests that traumatic experiences and chronic stress, which also affects 75% of Americans, don’t just take an emotional toll, but also deeply affect many biological systems. Part of this mechanism may involve the body’s chemical signaling systems. Research by neuroscientist Candace Pert and colleagues at the National Institutes of Health (NIH) demonstrated that neuropeptides and their receptors are distributed not only in the brain, but throughout the immune system and body as a whole. In other words, chronic activation of the stress response is not only a psychological experience: it is a whole-body event, with ongoing consequences for immune regulation, inflammation, gut health and other systems over time. The title of Bessel van der Kolk’s famous book, The Body Keeps the Score, captures this phenomenon: the body retains the biological consequences of what the nervous system has been asked to endure.
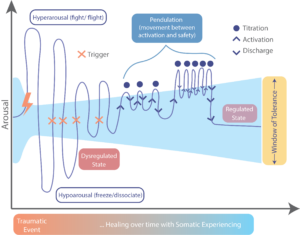
This understanding has given rise to a family of therapeutic approaches that support trauma survivors using body-based approaches. Somatic Experiencing (SE) is one such approach that has gained traction in recent decades. This approach differs from standard talk therapies, such that instead of asking a client to retell or revisit a traumatic experience, the SE practitioner directs the client’s attention toward what the body is doing and feeling in the current moment, specifically focusing on the subtle sensations of the body and areas of tension that exist beneath conscious thought. Psychologist Eugene Gendlin called this quality of bodily awareness the “felt sense,” a kind of physical knowing that precedes language. The aim of SE is to help the nervous system gradually complete the unresolved trauma responses that remain active in the body. One way SE does this is through pendulation, or the process of gently moving attention back and forth between sensations that feel difficult or activating and sensations that feel neutral or safe. This rhythm allows the nervous system to gradually expand its capacity to process what it has been holding without becoming overwhelmed. In doing so, SE works to restore the capacity to move between states of activation and rest in response to present circumstances rather than past ones, gradually expanding what is known as the window of tolerance. The work is slow and done incrementally, using an approach called titration to prioritize safety over intensity (see diagram below).
The clinical evidence for SE, while still developing, is encouraging. The first randomized controlled trial evaluating SE for PTSD, published in the Journal of Traumatic Stress in 2017, found significant reductions in post-traumatic symptom severity and depression following 15 weekly sessions with improvements that were sustained when participants were assessed again months later. A review of the growing body of SE research suggests promising effects across a range of physical and psychological symptoms, though the need for larger, more rigorous trials was highlighted. SE is one of several body-oriented approaches, alongside Eye Movement Desensitization and Reprocessing (EMDR), Sensorimotor Psychotherapy, trauma sensitive yoga, and mindfulness-based therapies. It’s important to understand that no single method works for everyone, and this remains an active area of research.
The underlying theme of these body-based approaches is the reframing of what healing from trauma really looks like. The experience of a traumatic event is not just a memory to be told, understood and analyzed, but also a physiological and biological state that needs to be addressed. To fully address the trauma, the nervous system needs to recognize and truly feel, as a biological reality, that the threat no longer exists. It is that shift from intellectual understanding to embodied knowing that allows the nervous system to settle and healing to be felt.
“The body always leads us home … if we can simply learn to trust sensation and stay with it long enough for it to reveal appropriate action, movement, insight or feeling” – Pat Ogden, Ph.D
Peer edited by: Rachel Sharp and Mary Kate Rinderle